Pharmacotherapeutic Group: Antibacterials for systemic use, combinations of penicillins including β-lactamase inhibitors.
ATC code: J01C R05.
Pharmacology: Pharmacodynamics: Mode of Action: Piperacillin/tazobactam (sterile piperacillin sodium/tazobactam sodium) is an injectable antibacterial combination consisting of the semisynthetic antibiotic piperacillin sodium and the β-lactamase inhibitor tazobactam sodium for intravenous administration. Thus, piperacillin/tazobactam combines the properties of a broad-spectrum antibiotic and a β-lactamase inhibitor.
Piperacillin sodium exerts bactericidal activity by inhibiting septum formation and cell wall synthesis. Piperacillin and other β-lactam antibiotics block the terminal transpeptidation step of cell wall peptidoglycan biosynthesis in susceptible bacteria by interacting with penicillin-binding proteins (PBPs), the bacterial enzymes that carry out this reaction.
In vitro, piperacillin is active against a variety of gram-positive and gram-negative aerobic and anaerobic bacteria.
Piperacillin has reduced activity against bacteria harboring certain β-lactamase enzymes, which chemically inactivate piperacillin and other β-lactam antibiotics. Tazobactam sodium, which has very little intrinsic antimicrobial activity, due to its low affinity for PBPs, can restore or enhance the activity of piperacillin against many of these resistant organisms. Tazobactam is a potent inhibitor of many class A β-lactamases (penicillinases, cephalosporinases and extended spectrum enzymes). It has variable activity against class A carbapenemases and class D β-lactamases. It is not active against most class C cephalosporinases and inactive against Class B metallo-β-lactamases.
Two features of piperacillin/tazobactam lead to increased activity against some organisms harboring β-lactamases that, when tested as enzyme preparations, are less inhibited by tazobactam and other inhibitors: tazobactam does not induce chromosomally mediated β-lactamases at tazobactam levels achieved with the recommended dosing regimen and piperacillin is relatively refractory to the action of some β-lactamases.
Like other β-lactam antibiotics, piperacillin, with or without tazobactam, demonstrates time-dependent bactericidal activity against susceptible organisms.
Mechanism of Resistance: There are three major mechanisms of resistance to β-lactam antibiotics: changes in the target PBPs resulting in reduced affinity for the antibiotics, destruction of the antibiotics by bacterial β-lactamases, and low intracellular antibiotic levels due to reduced uptake or active efflux of the antibiotics.
In gram-positive bacteria, changes in PBPs are a major mechanism of resistance to β-lactam antibiotics, including piperacillin/tazobactam. This mechanism is responsible for methicillin resistance in staphylococci and penicillin resistance in
Streptococcus pneumoniae as well as viridans group streptococci and enterococci. Resistance caused by changes in PBPs also occurs to a lesser extent in fastidious gram-negative species such as
Haemophilus influenzae and
Neisseria gonorrhoeae. Piperacillin/tazobactam is not active against strains in which resistance to β-lactam antibiotics is determined by altered PBPs. As indicated previously, there are some β-lactamases that are not inhibited by tazobactam.
MERINO Trial (blood stream infections due to ESBL producing organisms): In a prospective, randomized non-inferiority clinical trial, definitive (i.e., based on susceptibility confirmed in-vitro) treatment with piperacillin/tazobactam did not meet non-inferiority in regard to 30-day mortality in the treatment of blood stream infections due to ESBL producing E. coli or Klebsiella pneumoniae in critically ill adult patients. A total of 23 of 187 patients (12.3%) randomized to piperacillin/tazobactam met the primary outcome of mortality at 30 days compared with 7 of 191 (3.7%) randomized to meropenem (risk difference, 8.6% [1-sided 97.5% CI - ∞ to 14.5%]; P = 0.90 for non-inferiority). Clinical and microbiological resolution by day 4 occurred in 121 of 177 patients (68.4%) in the piperacillin/tazobactam group compared with 138 of 185 (74.6%), randomized to meropenem (risk difference, -6.2% [95% CI, -15.5 to 3.1%]; P = 0.19). The cause of the mortality imbalance is not clear. This study was not sponsored by Pfizer.
Methodology for Determining the
In Vitro Susceptibility of Bacteria to Piperacillin/Tazobactam: Susceptibility testing should be conducted using standardized laboratory methods, such as those described by the Clinical and Laboratory Standards Institute (CLSI). These include dilution methods (minimal inhibitory concentration [MIC] determination) and disk susceptibility methods. Both CLSI and the European Committee on Antimicrobial Susceptibility Testing (EUCAST) provide susceptibility interpretive criteria for some bacterial species based on these methods. It should be noted that for the disk diffusion method, CLSI and EUCAST use disks with different drug contents of piperacillin and tazobactam.
CLSI Reference Information: The CLSI interpretive criteria for susceptibility testing of piperacillin/tazobactam are listed in the following table:
(See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Standardized susceptibility test procedures require the use of quality control microorganisms to control the technical aspects of the test procedures. Quality control microorganisms are specific strains with intrinsic biological properties relating to resistance mechanisms and their genetic expression within the microorganism; the specific strains used for susceptibility test quality control are not clinically significant.
Organisms and quality control ranges for piperacillin/tazobactam to be utilized with CLSI methodology and susceptibility test interpretive criteria are listed in the following table:
(See Table 2.)
Click on icon to see table/diagram/image
EUCAST Reference Information: EUCAST has also established clinical breakpoints for piperacillin/tazobactam against some organisms. Like CLSI, the EUCAST MIC susceptibility criteria are based on a fixed concentration of 4 mg/L of tazobactam. However, for inhibition zone determination, the disks contain 30 μg of piperacillin and 6 μg of tazobactam. The EUCAST rationale document for piperacillin/tazobactam (Piperacillin-tazobactam. Rationale for the EUCAST clinical breakpoints, version 1.0. 22nd November 2010) states that breakpoints for
Pseudomonas aeruginosa apply to dosages of 4 g, 4 times daily, whereas the breakpoints for other organisms are based on 4 g, 3 times daily.
The EUCAST breakpoints for piperacillin/tazobactam are listed in the following table:
(See Table 3.)
Click on icon to see table/diagram/image
Per EUCAST, for species without piperacillin/tazobactam breakpoints, susceptibility in staphylococci is inferred from cefoxitin/oxacillin susceptibility. For groups A, B, C and G streptococci and
Streptococcus pneumoniae, susceptibility is inferred from benzylpenicillin susceptibility. For other streptococci, enterococci, and β-lactamase negative
Haemophilus influenzae, susceptibility is inferred from amoxicillin-clavulanate susceptibility. There are no EUCAST breakpoints for
Acinetobacter. The EUCAST rationale document for piperacillin/tazobactam states that in endocarditis caused by streptococci other than groups A, B, C and G and
S. pneumoniae, national or international guidelines should be referred to.
Quality control ranges for EUCAST susceptibility breakpoints are listed in the following table.
(See Table 4.)
Click on icon to see table/diagram/image
Antibacterial Spectrum (Groupings of relevant species according to piperacillin/tazobactam susceptibility): Commonly Susceptible Species: Aerobic gram-positive microorganisms: Enterococcus faecalis (ampicillin-or penicillin-susceptible isolates only), Listeria monocytogenes, Staphylococcus aureus (methicillin-susceptible isolates only), Staphylococcus spp., coagulase-negative (methicillin-susceptible isolates only), Streptococcus agalactiae (Group B streptococci)†, Streptococcus pyogenes (Group A streptococci)†.
Aerobic gram-negative microorganisms: Citrobacter koseri, Haemophilus influenzae, Moraxella catarrhalis, Proteus mirabilis.
Anaerobic gram-positive microorganisms: Clostridium spp., Eubacterium spp., Anaerobic gram-positive cocci††.
Anaerobic gram-negative microorganisms: Bacteroides fragilis group, Fusobacterium spp., Porphyromonas spp., Prevotella spp.
Species for which acquired resistance may be a problem: Aerobic gram-positive microorganisms: Enterococcus faecium, Streptococcus pneumoniae††, Viridans group streptococci†† .
Aerobic gram-negative microorganisms: Acinetobacter baumannii, Citrobacter freundii, Enterobacter spp., Escherichia coli, Klebsiella pneumoniae, Morganella morganii, Proteus vulgaris, Providencia spp., Pseudomonas aeruginosa, Serratia spp.
Anaerobic gram-positive microorganisms: Clostridium perfringens.
Anaerobic gram-negative microorganisms: Bacteroides distasonis, Prevotella melaninogenica.
Inherently resistant organisms: Aerobic gram-positive microorganisms: Corynebacterium jeikeium.
Aerobic gram-negative microorganisms: Burkholderia cepacia, Legionella spp., Stenotrophomonas maltophilia.
Other microorganisms: Chlamydophila pneumoniae, Mycoplasma pneumoniae.
† Streptococci are not β-lactamase producing bacteria; resistance in these organisms is due to alterations in penicillin-binding proteins (PBPs) and, therefore, piperacillin/tazobactam-susceptible isolates are susceptible to piperacillin alone. Penicillin resistance has not been reported in S. pyogenes.
†† Including Anaerococcus, Finegoldia, Peptococcus, Peptoniphilus and Peptostreptococcus spp. (CLSI M100 Ed. 29, 2019).
Pharmacokinetics: Distribution: Both piperacillin and tazobactam are approximately 30% bound to plasma proteins. The protein binding of either piperacillin or tazobactam is unaffected by the presence of the other compound. Protein binding of the tazobactam metabolite is negligible.
Piperacillin/tazobactam is widely distributed in tissues and body fluids including intestinal mucosa, gallbladder, lung, bile, and bone. Mean tissue concentrations are generally 50% to 100% of those in plasma.
Metabolism: Piperacillin is metabolized to a minor microbiologically active desethyl metabolite. Tazobactam is metabolized to a single metabolite that has been found to be microbiologically inactive.
Elimination: Piperacillin and tazobactam are eliminated via the kidney by glomerular filtration and tubular secretion.
Piperacillin is excreted rapidly as unchanged drug with 68% of the administered dose appearing in the urine. Tazobactam and its metabolite are eliminated primarily by renal excretion with 80% of the administered dose appearing as unchanged drug and the remainder as the single metabolite. Piperacillin, tazobactam, and desethyl piperacillin are also secreted into the bile.
Following administration of single or multiple doses of piperacillin/tazobactam to healthy subjects, the plasma half-life of piperacillin and tazobactam ranged from 0.7 to 1.2 hours and was unaffected by dose or duration of infusion. The elimination half-lives of both piperacillin and tazobactam are increased with decreasing renal clearance.
There are no significant changes in the pharmacokinetics of piperacillin due to tazobactam. Piperacillin appears to reduce the rate of elimination of tazobactam.
Special Populations: The half-lives of piperacillin and of tazobactam increase by approximately 25% and 18%, respectively, in patients with hepatic cirrhosis compared to healthy subjects.
The half-lives of piperacillin and tazobactam increase with decreasing creatinine clearance. The increase in half-life is two-fold and four-fold for piperacillin and tazobactam, respectively, at creatinine clearance below 20 mL/min compared to patients with normal renal function.
Hemodialysis removes 30% to 50% of piperacillin/tazobactam with an additional 5% of the tazobactam dose removed as the tazobactam metabolite. Peritoneal dialysis removes approximately 6% and 21% of the piperacillin and tazobactam doses, respectively, with up to 18% of the tazobactam dose removed as the tazobactam metabolite.
Toxicology: Preclinical safety data: Carcinogenicity: Carcinogenicity studies have not been conducted with piperacillin, tazobactam, or the combination.
Mutagenicity: Piperacillin/tazobactam was negative in microbial mutagenicity assays. Piperacillin/tazobactam was negative in the unscheduled DNA synthesis (UDS) test. Piperacillin/tazobactam was negative in a mammalian point mutation (Chinese hamster ovary cell hypoxanthine phosphoribosyltransferase [HPRT]) assay.
Piperacillin/tazobactam was negative in a mammalian cell (BALB/c-3T3) transformation assay.
In vivo, piperacillin/tazobactam did not induce chromosomal aberrations in rats dosed intravenously.
Piperacillin was negative in microbial mutagenicity assays. There was no DNA damage in bacteria (Rec assay) exposed to piperacillin. Piperacillin was negative in the UDS test. In a mammalian point mutation (mouse lymphoma cells) assay, piperacillin was positive. Piperacillin was negative in a cell (BALB/c-3T3) transformation assay.
In vivo, piperacillin did not induce chromosomal aberrations in mice dosed intravenously.
Tazobactam was negative in microbial mutagenicity assays. Tazobactam was negative in the UDS test. Tazobactam was negative in a mammalian point mutation (Chinese hamster ovary cell HPRT) assay. In another mammalian point mutation (mouse lymphoma cells) assay, tazobactam was positive. Tazobactam was negative in a cell (BALB/c-3T3) transformation assay. In an in vitro cytogenetics (Chinese hamster lung cells) assay, tazobactam was negative. In vivo, tazobactam did not induce chromosomal aberrations in rats dosed intravenously.
Reproductive Toxicity: In embryo-fetal development studies, there was no evidence of teratogenicity following intravenous administration of tazobactam or the piperacillin/tazobactam combination; however, in rats there were slight reductions in fetal body weight at maternally toxic doses.
Intraperitoneal administration of piperacillin/tazobactam was associated with slight reductions in litter size and an increased incidence of minor skeletal anomalies (delays in bone ossification) at doses that produced maternal toxicity. Peri-/postnatal development was impaired (reduced pup weights, increase in still birth, increase in pup mortality), concurrent with maternal toxicity.
Impairment of Fertility: Reproduction studies in rats revealed no evidence of impaired fertility due to tazobactam or piperacillin/tazobactam when administered intraperitoneally.





 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image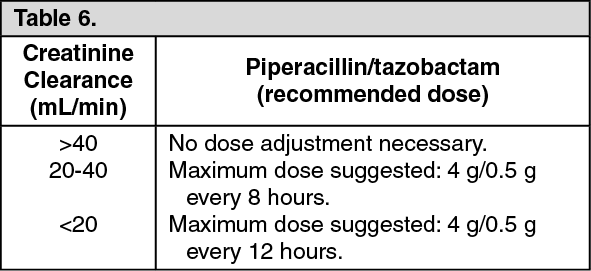 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image4e935aa6-38e3-4f33-92a5-9faa000a157b.GIF)

 Sign Out
Sign Out
